In this issue:
To Splint or Not to Splint: Two Approaches to Multi-Unit Implant Restorations
Author


Note: The Hahn Tapered Implant System is now known as the Glidewell HT Implant System
When a patient’s treatment involves more than one implant in an edentulous space, the clinician must make a decision: Should multiple single-unit restorations be used, or would a splinted restoration be a better choice? The answer to this question is dependent on a variety of factors related to the particular patient and the case at hand. Here are the most important considerations that can help you make the decision and guide your restorative planning.
ADVANTAGES OF FREE-STANDING RESTORATIONS
Patient Preference
If you ask patients, they are likely to tell you that they prefer separate crowns rather than a splinted restoration, for the simple reason that they’re most familiar with the feeling of individual teeth. While we as clinicians know that splinted restorations may feel unfamiliar to the patient at first but will quickly feel comfortable and natural, the patient’s uncertainty should not be disregarded. Patients who feel they are participating in the decisions about their treatment plan are more likely to be satisfied with the final outcome, and thus more likely to continue proper maintenance of the implants and follow through with continuing care.
Cleansability
Splinted restorations require the patient to master more demanding techniques for interproximal cleaning. Many patients will be noncompliant because they may have difficulty learning to use these new hygiene aids and methods, and the cleanliness and long-term health of the restoration will suffer in such cases.
What’s more, there is evidence to show that, among screw-retained restorations, those that are unsplinted may sometimes stay cleaner and healthier than splinted versions due to a fundamental difference in the implant-abutment connection interface. Unsplinted screw-retained restorations are fabricated with anti-rotational (engaging) implant abutments, which form a strong mechanical connection due to the interlocking geometry and machined fit created by the manufacturer. This minimizes microgaps and thus limits the amount of bacterial infiltration that can occur, resulting in a healthier implant at the bone level.1 Splinted screw-retained restorations are often constructed with rotational (non-engaging) implant abutments to allow for ease of multi-unit insertion. This design does not create the same level of mechanical seal around the interface. This issue, of course, can be mitigated in two different ways: For a screw-retained restoration, multi-unit abutments can be used to better engage the interface; cemented restorations can also be fabricated on custom abutments.
THE CASE FOR SPLINTED RESTORATIONS
Favorable Load Distribution
The ability to withstand non-vertical occlusal forces is a key advantage to the use of splinted restorations. Because the restorations are attached as a single piece, any functional force is spread across the greater surface area of all of the units of the restoration. This creates a more favorable load distribution that minimizes stress on the bone and maximizes the stability of the restoration, which leads to better long-term survival rates and less bone loss over the long term.2
Stability in Compromised Patients
For patients with compromised bone quality and quantity, or in cases where the patient’s surrounding teeth have short or extremely tapered roots or are excessively mobile, a splinted restoration is typically indicated for stability reasons. Due to the better load distribution explained above, splinted restorations can help compensate for a lack of stability created by the patient’s compromised dental health.
CASE REPORT
In this case, the patient presented with pain in the lower left posterior quadrant of her mouth. Upon examination, it was discovered that she had two failing premolars side by side, both of which had received cast restorations several years in the past. Failure was due to recurrent decay beneath those restorations. Her molar #19 had also been removed several years ago, resulting in a span where three adjacent teeth required replacement.
The patient selected implant treatment to replace her teeth. Screw-retained crowns were chosen instead of a cementable restoration, primarily due to the ease of retrievability afforded by screw retention. Because the posterior location of the restorations required resistance to occlusal forces as well as acceptable esthetics, I selected BruxZir® zirconia as the material; its high flexural strength and natural translucency fulfilled both requirements.

Figure 1: The patient presented with pain in her lower left posterior quadrant caused by the terminal state of her bicuspids. Upon removal, the recurrent decay of these teeth beneath their previously placed cast restorations was visibly evident.
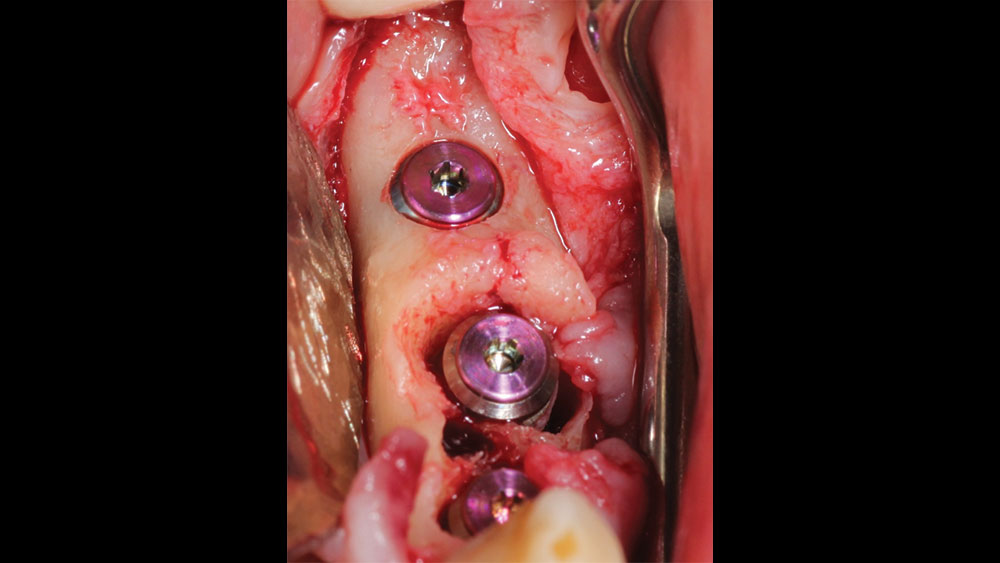
Figure 2: Once the failing teeth were removed, a surgical flap was created and three 4.3 mm Hahn™ Tapered Implants (Glidewell Direct; Irvine, Calif.) were placed into the site. Cover screws were then connected to the implants, and the surgical flap was sutured back into place and given three months to heal prior to the next step.

Figure 3: Three months after implant placement, the cover screws were removed and healing abutments were placed. The site was then given another three months to heal.
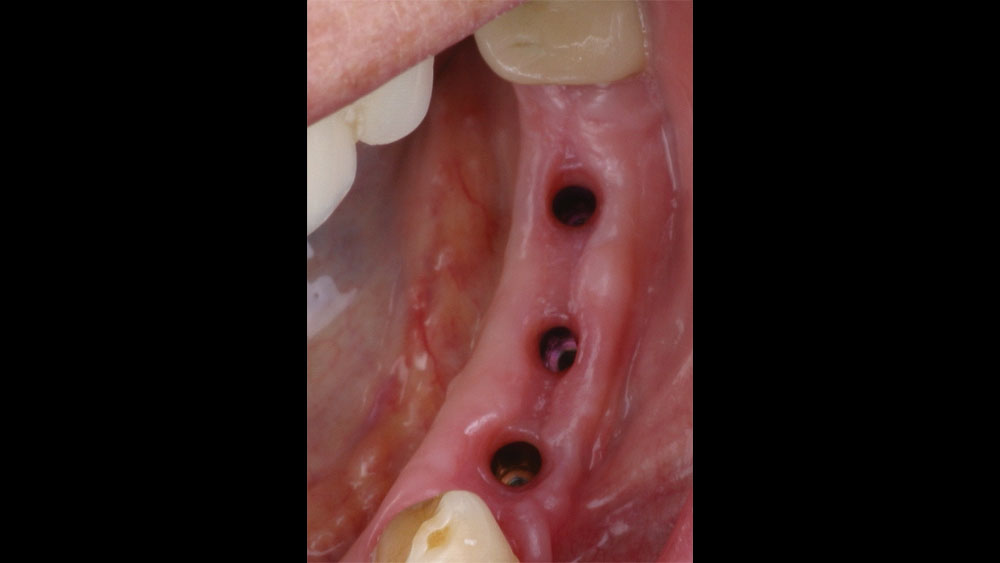
Figure 4: Six months after implant placement, the healing abutments were removed so that final impressions could be taken. The soft tissue showed good health.

Figure 5: Closed-tray impression copings were connected to the implants in order to take the final impressions

Figure 6: Three separate BruxZir Full-Strength Solid Zirconia screw-retained crowns were created by Glidewell Laboratories. Advantages of these unsplinted restorations include the fact that they were esthetically what the patient desired and would be easier for her to clean. Another advantage was the hex connections of the implant screws, which would create a strong mechanical connection and minimize microgaps that might allow bacterial infiltration. The crowns were placed in the patient’s mouth and evaluated for final adjustments. The fit, occlusion and esthetics were excellent and the prognosis for long-term success looked good.

Figure 7: This final radiograph shows the integrated Hahn Tapered Implants as well as the individual BruxZir crowns after delivery, both of which contributed to an outcome that met the unique needs of the case.
The question then became whether to use a splinted restoration in the form of a BruxZir screw-retained bridge, or unsplinted BruxZir screw-retained crowns. An assessment of this patient, as well as the pros and cons of both restoration types as previously outlined, led to the decision that an unsplinted restoration was the preferred treatment in this case. The key factors in this choice were as follows:
- The opposing dentition for this patient was a full denture. This meant that the extra stability and bite force distribution provided by a splinted restoration was not a requirement here, and I was able to remove that consideration from the equation.
- The patient had adjacent teeth on both sides of the implants, which would assist in the distribution of occlusal loads.
- As illustrated by her dental history, the patient had experienced several issues with decay in this area of her mouth. This indicated strongly that the patient most likely had challenges keeping the area clean, and any restoration that would limit her ability to clean the area could be problematic.
CONCLUSION
Cases involving multiple adjacent restorations will always raise the question of whether a splinted or unsplinted approach is the better option. By carefully analyzing the pros and cons of each restoration type and weighing those factors against the particular considerations and priorities involved in that patient’s individual case, the informed clinician can make a decision that’s best for long-term survivability as well as patient health, comfort and happiness.
References
- ^Hermann JS, Schoolfield JD, Schenk RK, Buser D, Cochran DL. Influence of the size of the microgap on crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged implants in the canine mandible. J Periodontol. 2001 Oct;72(10):1372-83.
- ^Lemos CAA, Verri FR, Santiago Junior JF, de Souza Batista VE, Kemmoku DT, Noritomi PY, Pellizzer EP. Splinted and nonsplinted crowns with different implant lengths in the posterior maxilla by three-dimensional finite element analysis. J Healthc Eng. 2018 Sep 3;2018:3163096.